Excess Dorsiflexion
Understanding how too much upward ankle movement during weight-bearing can affect posture, balance, and gait, and how the right support can help guide more efficient movement through the ankle, knee, and hip.
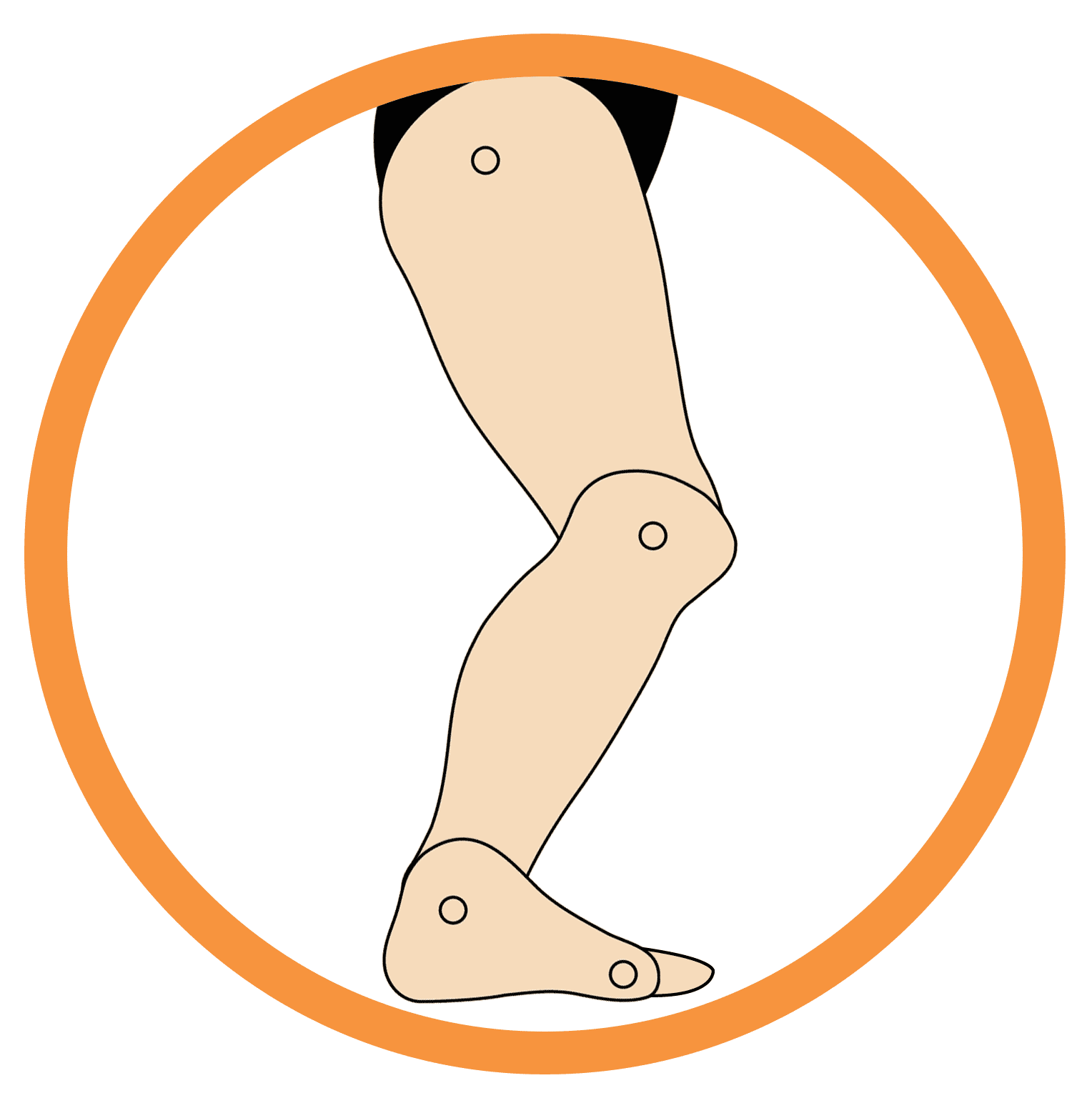
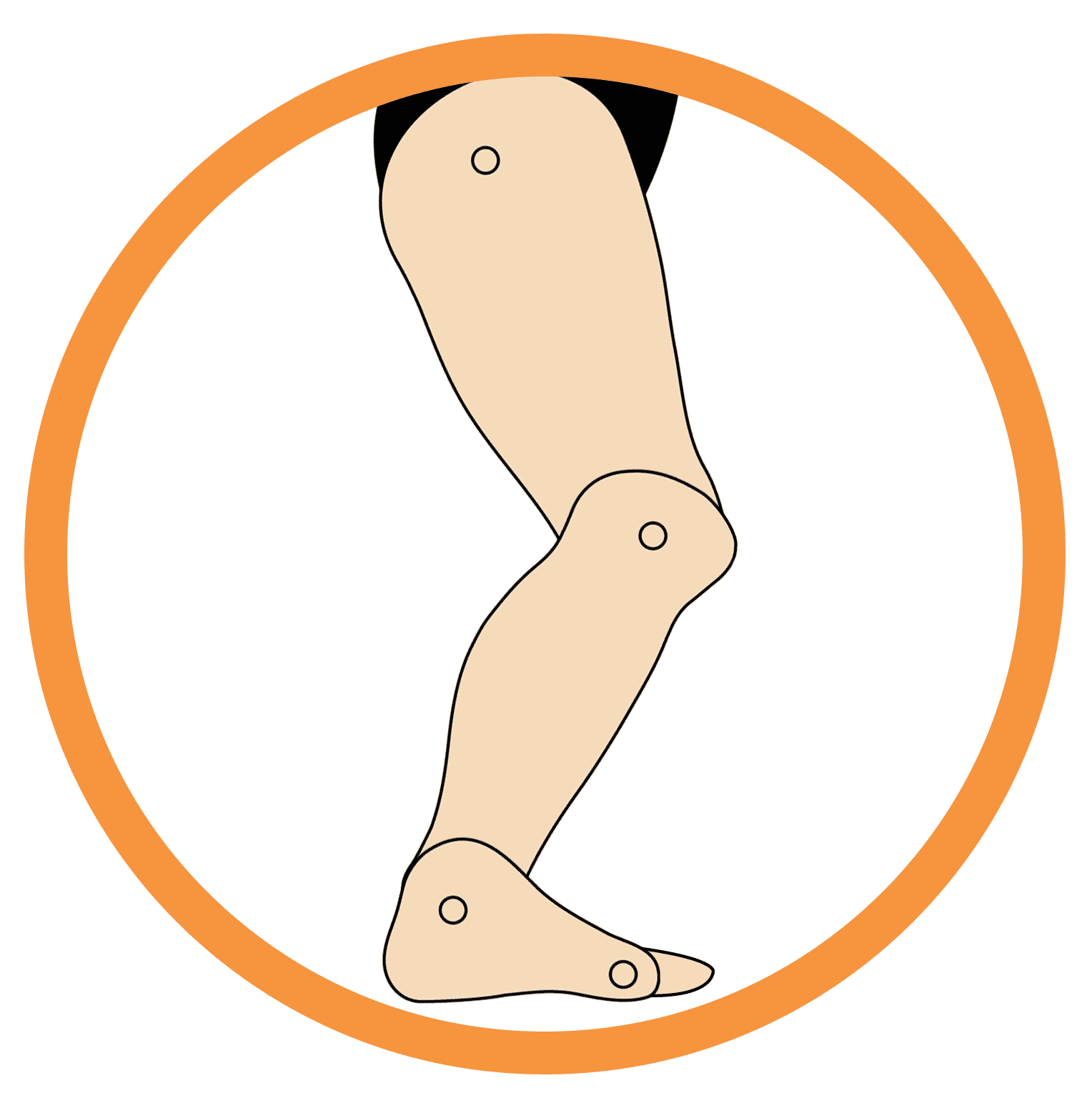
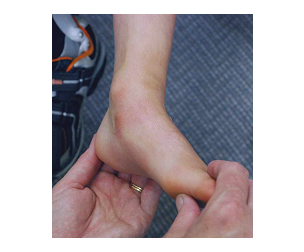
What Is Excess Dorsiflexion?
Excess Dorsiflexion describes a movement pattern where the ankle bends upward more than expected during weight-bearing. This is often seen together with increased bending at the knees and hips, creating a crouched posture during standing and walking.
This pattern is commonly linked to muscle weakness or low tone rather than joint restriction. Instead of the ankle providing a stable base during stance, it continues to collapse upward, which shifts more demand to the knees and hips. Over time, that can affect endurance, balance, and movement efficiency. Excess Dorsiflexion is not just an ankle issue. It reflects how ankle control, knee flexion, and hip positioning work together during gait.
Understanding the terminology is essential:
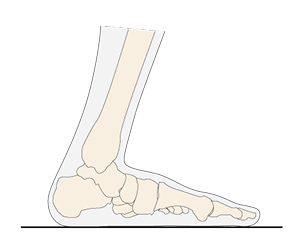
Dorsiflexion
Lifting the foot upward toward the shin.
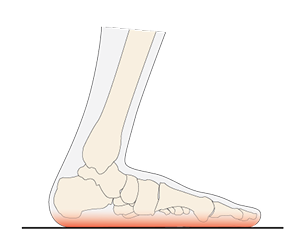
Weight-Bearing
When the foot is on the ground supporting body weight.
Low Tone
Reduced background muscle activity that can affect stability.
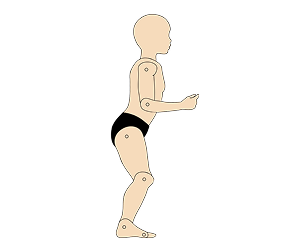
Crouched Posture
A walking pattern with persistent bending at the ankles, knees, and hips.
Severity Assessment
Q1. Select what ankle and knee flexion looks like

Q2. Select the frequency
Total Score
This Assessment is not a medical diagnosis. If you have any questions, please seek out a professional medical clinician.
Suggested Bracing Options









Indicators of Success: How to Know It's Working
Progress is often reflected in how posture and movement feel during daily activity, not just in joint angles. Signs that support is helping may include:
Improved upright posture during stance
Reduced crouching during walking
More effective use of knee and hip motion
Increased endurance during daily activities
Greater confidence during standing and walking
If the ankle continues to collapse during stance, discomfort develops at the knee, hip, or ankle, or tolerance changes with growth or activity level, the support plan may need to be reviewed.
Supporting the Journey: Family and Team Collaboration
Excess Dorsiflexion is best understood as a whole-body movement pattern rather than only an ankle presentation. That means progress is easier to track when families, clinicians, and educators look at posture, endurance, comfort, and confidence together.
Observing posture regularly
Watch how standing and walking look across daily routines, not just in one setting.
Sharing observations across environments
Feedback from home, clinic, and school helps build a clearer picture of what is improving and what still needs support.
Focusing on comfort and endurance
Success is not only about alignment. It is also about how movement feels and how long it can be sustained.
Celebrating progress in participation
Even small improvements in posture, stability, or willingness to move can be meaningful.
As needs change over time, regular follow-up helps ensure the support continues to match comfort, fit, and functional goals.
Common Questions (FAQ)
In many ways, yes. Instead of staying on the toes, the ankle collapses upward too much during stance.
The knees and hips bend to compensate for a lack of stability at the ankle during weight-bearing.
The goal is to improve how motion is shared across the ankle, knee, and hip, not to restrict overall movement unnecessarily.
Not necessarily. The level and duration of support may change over time as strength, control, and functional needs change.
Yes. Internal or external foot rotation is often used as a compensation strategy when stability is limited.
The source describes severity in mild, moderate, and strong terms based on how consistently crouching and excess dorsiflexion appear during stance and gait, though it also notes that detailed clinical benchmarks still need to be added.